
Perspective
- Introduction to HIV/AIDs
- Distribution and determinants
- Signs and symptoms
- Major risk factors for HIV/AIDS
- Screening and diagnosis
- Impact of nutritional intervention for HIV + ART efficacy
- Healthcare systems
- Intervention summary
The emergence HIV infection in the 1980s marked a critical point in public health. In 1981, HIV was officially recognized as the primary etiological factor responsible for acquired immunodeficiency disease (AIDS). During this year there was a surge in the number of AIDS cases among a particular demographic, notably young, homosexual men, who displayed unusual opportunistic infections and symptoms. 4 Several countries, including South Africa, Russia, USA and Israel have grappled with the complex challenge of HIV infection rates. Since the 1990’s these countries witnessed a steady escalation in the prevalence of infection until the early 2000s, when there began a gradual decline in infection rate.6 This decline can be attributed in part to multifaceted public health campaigns aimed at mitigating the risk of HIV infection. Primary and secondary prevention programs involve pre-exposure prophylaxis, condom availability, and better coverage for ART use in HIV-positive mothers-to-child-transmission.5
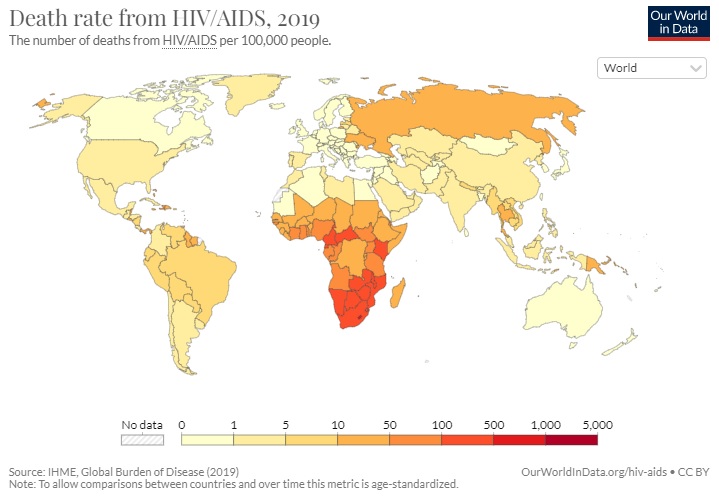
There were an estimated 38.0 million people living with HIV at the end of 2019.(WHO)

Human immunodeficiency virus, otherwise known as HIV, is a virus that attacks the body’s immune system, by gradually destroying the white blood cells called CD4 cells or helper T cells, responsible for fighting infection.1 Pathophysiologically, HIV is able to infiltrate CD4 cells by interacting with the cell receptors known as CD4, CCR5 and CXCR4, using its outer layer proteins GP120 and Gp41, allowing HIV to fuse with the cell.2 After entering the cell HIV causes a cascade of transcriptive processes to convert its RNA into viral DNA, due to its molecular structure containing reverse transcriptase enzymes.3 Reverse transcription being an important phase within retroviral replication.2,3 When left untreated HIV can progresses into the most severe phase of the infection, known as acquired immunodeficiency disease (AIDS), in addition to leaving the host susceptible to other comorbidities and a heightened risk of mortality due to a severely damaged immune system.1
Distribution and determinants of HIV infection within populations.
-
Prevalence: HIV is a global pandemic, with varying prevalence rates in different regions. Sub-Saharan Africa has the highest prevalence, with a significant burden of HIV infections. Other regions, including parts of Asia, the Americas, and Eastern Europe, also have significant HIV rates.
-
Incidence: Globally, HIV incidence has decreased in recent years, thanks to prevention efforts and antiretroviral therapy (ART) access.
-
Demographics: HIV affects individuals of all ages, genders, and sexual orientations. However, certain demographic groups are disproportionately affected. Key populations at higher risk include men who have sex with men, people who inject drugs, sex workers, and transgender individuals.
-
Transmission: Sexual transmission remains the primary mode of HIV transmission worldwide. However, in some regions, injecting drug use is a significant driver of new infections. Mother-to-child transmission during childbirth or breastfeeding is another important mode of transmission, although it is preventable with appropriate interventions.
-
Antiretroviral Therapy (ART): The introduction of ART has transformed the HIV epidemic. It has improved the prognosis for individuals living with HIV, reduced AIDS-related deaths, and lowered the risk of transmission to uninfected partners. Access to ART varies globally, with efforts to scale up treatment in resource-limited settings.
-
Prevention: HIV prevention strategies include condom use, harm reduction programs for drug users, needle exchange programs, pre-exposure prophylaxis (PrEP) for high-risk individuals, and campaigns to promote safe sex and HIV testing.
-
Stigma and Discrimination: Stigma and discrimination against people living with HIV continue to be significant barriers to prevention, care, and treatment efforts. Reducing HIV-related stigma is a key focus of many public health initiatives.
-
Global Response: The global response to HIV/AIDS is coordinated by organizations such as UNAIDS and involves governments, NGOs, healthcare providers, and communities. The response includes funding for prevention, treatment, research, and advocacy.
In summary, the epidemiology of HIV encompasses the distribution, determinants, and dynamics of HIV infection within populations. Understanding these factors is crucial for designing effective strategies to prevent new infections, provide care and treatment for those living with HIV, and ultimately control the global HIV/AIDS pandemic.

HIV Infection Symptoms:
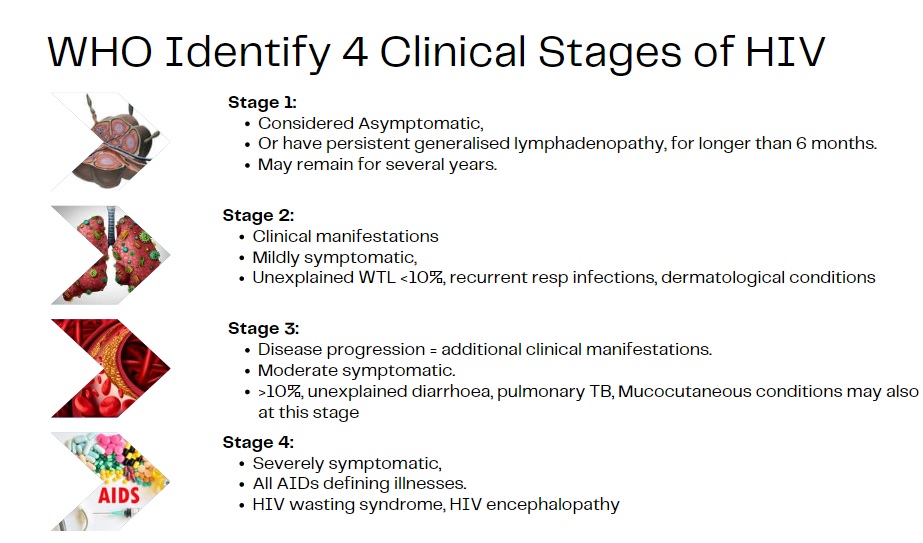
During the acute phase of HIV infection, a person may present with persistent flu-like symptoms. The later stages of infection may involve mucocutaneous symptoms, unintentional weight loss >10%, chronic fever, diarrhea and bacterial infections.7,8
Stage 4 based on the WHO clinical criteria identifies AIDS, which is accompanied with wasting syndrome, encephalopathy, and risks to certain cancers.8
-
Acute Retroviral Syndrome (ARS): Shortly after HIV infection, some individuals experience flu-like symptoms, often mistaken for a common viral illness.
These symptoms may include:- Fever
- Fatigue
- Swollen lymph nodes
- Sore throat
- Muscle and joint pain
- Rash
- Headache
-
Asymptomatic Stage: Many people with HIV do not experience any symptoms for several years after infection. During this time, the virus is actively multiplying in the body.
Progression to AIDS Symptoms:
-
Advanced HIV Infection (Symptomatic HIV): As the immune system deteriorates, individuals may experience symptoms and infections, such as:
- Chronic diarrhea
- Weight loss
- Recurrent fever
- Oral or genital ulcers
- Thrush (oral candidiasis)
- Night sweats
- Fatigue
- Skin problems, such as rashes and lesions
-
Opportunistic Infections: When the immune system is severely compromised, opportunistic infections, which are typically controlled by a healthy immune system, can occur.
These include:- Pneumocystis pneumonia (PCP)
- Tuberculosis (TB)
- Cytomegalovirus (CMV) infection
- Cryptococcal meningitis
- Toxoplasmosis
- Candidiasis of the esophagus, trachea, bronchi, or lungs
-
Opportunistic Cancers: People with AIDS have a higher risk of certain cancers, including:
- Kaposi's sarcoma
- Non-Hodgkin lymphoma
- Invasive cervical cancer
-
Neurological Symptoms: AIDS can lead to neurological complications, such as:
- Cognitive impairment
- Memory problems
- Neuropathy (nerve damage)
- Muscle weakness
-
Wasting Syndrome: Severe weight loss and muscle atrophy, known as wasting syndrome, can occur in advanced HIV infection.
-
HIV-Related Complications: Individuals with advanced HIV infection may experience a range of complications affecting the organs and systems of the body, including the cardiovascular system, liver, kidneys, and respiratory system.
It's important to note that the progression from HIV to AIDS is not linear, and the timeline varies widely among individuals. With early diagnosis and appropriate medical care, many people living with HIV can delay or prevent the progression to AIDS. Antiretroviral therapy (ART) is the primary treatment for HIV and AIDS, and it can help manage the virus, restore immune function, and reduce the risk of opportunistic infections and complications. Regular medical monitoring and adherence to treatment are crucial for the well-being of individuals living with HIV.

Several factors have contributed to the global spread of HIV.
- Unprotected anal or vaginal sex
- Injecting drug use
- The exchange of contaminated needles
- Breast feeding by HIV positive mother
- Exchanging blood products
There is an increased risk associated with another sexually transmitted disease (STI) such as gonorrhoea, bacterial vaginosis, syphillis, chlamydia. Social and economic factors, including poverty, lack of access to healthcare, and stigma associated with HIV, have also played a role in the spread of the virus.

Testing
-
Types of HIV Tests:
- Antibody Tests: These tests detect antibodies produced by the body in response to HIV infection. Common antibody tests include ELISA and rapid antibody tests. These tests are used for initial screening.
- Nucleic Acid Tests (NATs): NATs detect the genetic material (RNA or DNA) of the virus itself. They are more sensitive and can detect HIV earlier than antibody tests. NATs are often used for confirmation of HIV infection.
-
Point-of-Care Testing: Rapid HIV tests can provide results in as little as 20-30 minutes. They are often used in clinics, mobile testing units, and community-based settings.
HIV Diagnosis:
-
Initial Positive Test: If an initial HIV screening test is positive, it does not necessarily mean the individual has HIV. It means further testing is needed to confirm the diagnosis.
-
Confirmatory Testing: To confirm HIV infection, a second, different type of test is conducted. This is often a Western blot test or an indirect immunofluorescence assay (IFA). If both the initial and confirmatory tests are positive, the diagnosis is confirmed.
-
CD4 Cell Count and Viral Load Testing: After an HIV diagnosis is confirmed, additional blood tests are performed to assess the individual's immune status and viral load. The CD4 cell count measures the health of the immune system, while viral load testing quantifies the amount of HIV in the blood.
-
Staging: Based on CD4 cell count and clinical symptoms, HIV is categorized into stages (e.g., stage 1, 2, 3, or AIDS). Staging helps determine the urgency and type of treatment needed.

The treatment of HIV involves antiretroviral therapy (ART), with the primary purpose of sustaining viral suppression and reducing key complications associated with HIV.10 Regular monitoring of viral load and CD4 cell count is recommended to ensure ART efficacy.11 ART is prescribed to all patients diagnosed with HIV irrespective of their VL and CD4 cell count.10 ART is not a monotherapy but rather consists of a combination of medicines as part of a regimen aimed at targeting the different stages of the HIV replication cycle.12 A normal CD4 cell count is considered between 500-1500 cells/mm3 and levels <200 cells/mm3 may be associated with opportunistic infections and AIDS diagnosis. ART therapy should be initiated before abnormal readings. ART has significantly improved the prognosis and quality of life for people living with HIV. While ART is highly effective in suppressing the virus and restoring immune function, it can have several nutritional implications.13-18
-
Metabolic Changes: Some antiretroviral medications, particularly older drugs like protease inhibitors, can lead to metabolic changes in the body. These changes may include:
- Increased Fat Redistribution: Lipodystrophy syndrome can cause fat accumulation in certain areas (lipohypertrophy) and fat loss in others (lipoatrophy).
- Changes in Lipid Profiles: ART can affect lipid levels, leading to elevated cholesterol and triglycerides.
-
Bone Health: Some studies suggest that certain antiretroviral drugs may be associated with a higher risk of bone density loss (osteopenia and osteoporosis). Adequate calcium and vitamin D intake, along with weight-bearing exercise, can help support bone health.
-
Gastrointestinal Symptoms: ART can sometimes cause gastrointestinal side effects, such as nausea, diarrhea, or loss of appetite. These symptoms can impact nutritional intake and absorption.
-
Increased Nutritional Needs: HIV infection itself and the body's response to inflammation can increase energy expenditure and nutrient requirements. People on ART may need more calories and nutrients to support their immune system and overall health.
-
Interaction with Food: Some antiretroviral drugs need to be taken with food to enhance absorption and reduce side effects. It's important for individuals to follow their healthcare provider's instructions regarding food and medication interactions.
-
Potential Drug-Nutrient Interactions: ART may interact with certain nutrients or dietary supplements. For example, some drugs can affect the metabolism of specific vitamins or minerals, potentially leading to deficiencies. Healthcare providers should monitor and manage these interactions.
-
Liver Function: Liver function should be monitored regularly in individuals taking ART, as certain medications can affect liver enzymes. Adequate nutrition and avoidance of excessive alcohol intake are essential for liver health.
-
Immune Function: Proper nutrition is crucial for supporting immune function. A well-balanced diet with adequate protein, vitamins, and minerals can help maintain immune health.
-
Adherence and Nutrition: Maintaining good nutritional status can positively impact adherence to ART. People who feel healthy and have a well-balanced diet may be more likely to take their medications as prescribed.
-
Management of Side Effects: For individuals experiencing side effects from ART, such as nausea or loss of appetite, nutritional strategies such as eating smaller, more frequent meals and staying hydrated can be helpful.
-
Nutritional Counseling: Many HIV care programs include nutritional counseling as part of comprehensive care. Registered dietitians or nutritionists can assess individual nutritional needs, provide guidance on dietary choices, and address specific concerns related to HIV and ART.
The handling of HIV/AIDs may be due to a countries' available resources and the funding/structure of healthcare systems and initiation of public health campaigns. However, heightened instances of HIV/AIDS can be examined within Southeast Asian countries predominantly due to the limited resources and funds available to the countries' respected health care system.5 For the purpose of this case, the nutritional assessment will be focused on a South African patient. However, before undertaking the data collection for the nutritional assessment, it is important to understand South Africa's socioeconomic status and further the health care system, to gain knowledge about how to appropriately develop a management plan that would be suitable to the patient based on their environmental background.

The South African health care system, similar to most countries, can be divided into a public health system and a private health system. A recent consensus report by the South African Lancet National Commission revealed that the public health system is grossly inadequate, especially within rural areas.19 There is also a quadruple burden of disease associated with HIV/AIDs in combination with a higher burden of tuberculosis. This is further complicated by high levels of poverty and unemployment/social-economic inequities, which mean that the majority of the South African population, particularly in rural areas, are dependent on the public health system.19

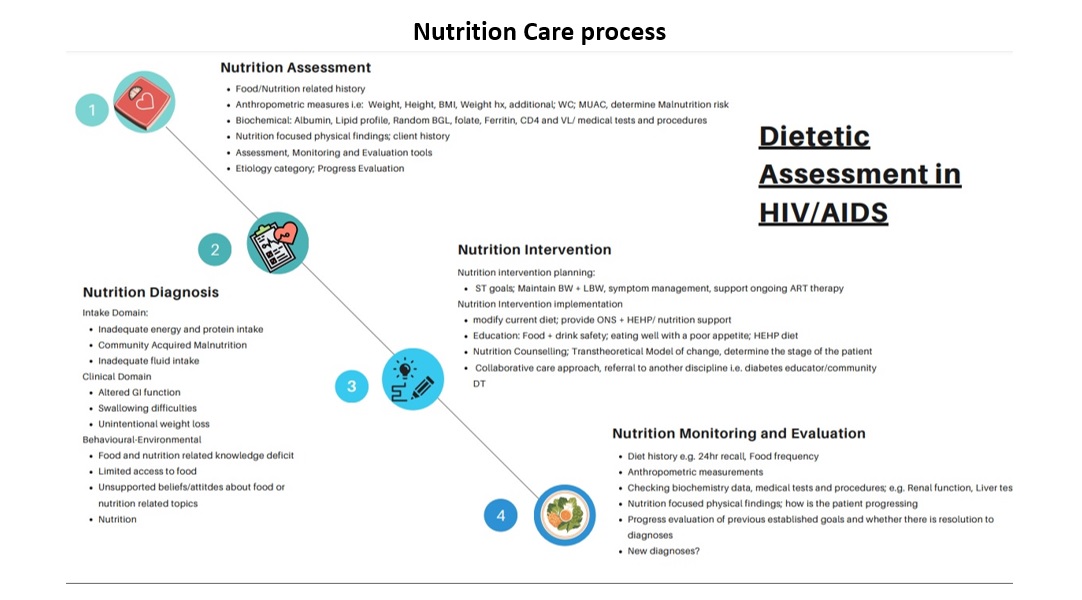
The nutritional management of HIV may be considered complex, as there is a clear established relationship between HIV and malnutrition. Malnutrition contributes to weight loss, nutritional deficiencies, muscle, and fat wasting, further lowering the immune system, consequently resulting in HIV progression leading to increased metabolic demands and nutritional requirements.20 This is further complicated with food insecurity.21
When food accessibility becomes a barrier to nutritional intake, a cascade of nutritional implications occurs that may inevitably reduce ART drug efficacy and increase the progression of HIV to AIDs.17,18,22 In addition, this mismanagement of nutrition may further cause significant weight loss, whereby the body will be unable to fight HIV/AIDs and cause a vicious cycle to the patients' overall health.18 Poverty and food insecurity are some of the key challenges associated with the deteriorating health seen within HIV/AIDS. Dietitians are therefore heavily integrated within the multidisciplinary team for HIV/AIDs. Some of the key nutritional management strategies may surround correcting malnutrition and micro/macronutrient deficiencies, providing tailored education to the patient on how to best support their condition and to further address the additional clinical manifestations associated with HIV itself.
Counselling strategies tailored to nutritional education in HEHP can help provide the patient with the relevant knowledge and tools to sustain desirable behaviour change and address barriers associated with HIV/AIDS, such as poor appetite, further supporting them to prevent complications and further progression to the disease.
References
- World Health Organization (WHO). HIV/AIDS [Internet]; Geneva, WHO [Updated 2023; cited 2023 Apr 24]. Available from: https://www.who.int/health-topics/hiv-aids#tab=tab_1
- Sarafianos ST, Marchand B, Das K, Himmel D, Parniak MA, Hughes SH et al. Structure and function of HIV-1 reverse transcriptase: molecular mechanisms of polymerization and inhibition. J Mol Biol [Internet]; [cited 2023 April 24]; 385(3):693-713. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2881421/
- (Hu WS and Hughes, HIV-1 Reverse Transcription. Cold Spring Harb Perspect Med [Internet]. 2012; 2(10): a006882. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3475395/
- Sharp PM, Hahn BH. Origins of HIV and the AIDS Pandemic. Cold Spring Harb Perspect Med [Internet]. 2011 Sep [cited 2023 Apr 24]; 1(1): a006841. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3234451/#A006841C45
- Govender RD, Hashim MJ, Khan MAB, Mustafa H, Khan G. Global Epidemiology of HIV/AIDS: A Resurgence in North America and Europe. J Epidemiol Glob Health [Internet]. 2021 Sep [cited 2023 April 26]; 11(3): 296-301. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8435868/#B3
- Roser M, Ritchie H- HIV/AIDS [Internet]. UK: Global Change Data Lab; 2014 [updated 2019 Nov; cited 2023 April 26]. Available from: https://ourworldindata.org/hiv-aids#citation
- Kovarik CL. The WHO clinical staging system for HIV/AIDS. AMA J Ethics [Internet]. 2010 March [cited 2023 April 23];12(3):202-6. Available from: https://journalofethics.ama-assn.org/article/who-clinical-staging-system-hivaids/2010-03
- Morgan D, Mahe C, Mayanja B, Whitworth JA. Progression to symptomatic disease in people infected with HIV-1 in rural Uganda: prospective cohort study. BMJ [Internet]. 2002 Jan [cited 2023 Apr 24]; 326(7331):193-197. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC64788/
- Centers for Disease Control and Prevention (CDC). HIV Testing [Internet]. USA; [Updated 2022 June 9; cited 2023 April 26]. Available from: https://www.cdc.gov/hiv/testing/index.html#:~:text=An%20antigen%2Fantibody%20test%20performed,to%2090%20days%20after%20exposure.
- National Institutes of Health (NIH). HIV Treatment [Internet]. USA, NIH [Updated 2021 Aug 16; cited 2023 Apr 26]. Available from: https://hivinfo.nih.gov/understanding-hiv/fact-sheets/hiv-treatment-basics#:~:text=The%20treatment%20for%20HIV%20is,medicines%20as%20soon%20as%20possible.
- World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach [Internet]. World Health Organization; 2016 [cited 2023 Apr 26]. Available from: https://apps.who.int/iris/bitstream/handle/10665/208825/97892?sequence=1 .
- Hughes Y, Tomlins L, Usherwood T. Prescribing for patients taking antiretroviral therapy. Aust Prescrib [Internet]. 2022 June [cited 2023 April 23;45(3):80. Available from: https://www.nps.org.au/australian-prescriber/articles/prescribing-for-patients-taking-antiretroviral-therapy
- Battistini Garcia SA, Guzman N. Acquired Immune Deficiency Syndrome CD4+ Count. [Updated 2022 Aug 8’ cited: 2023 Apr 28th]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513289/
- Wassner C, Bradley N, Lee Y. A Review and Clinical Understanding of Tenofovir: Tenofovir Disoproxil Fumarate versus Tenofovir Alafenamide. J Int Assoc Provid AIDS Care [Internet]. 2020 Jan-Dec [cited 2023 April 24]; 19. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7163232/
- Holec AC, Mandal S, Prathipati PK and Destache CJ. Nucelotide Reverse Transcriptase Inhibitors: A Thorough Review, Present Status and Future Perspective as HIV Therapeutics. Curr HIV Res. 2017 [cited 2023 April 24]; 15(6): 411-421. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219633/
- Harding BN, Whitney BM, Nance RM, Crane HM, Burkholder G, Moore RD, et al. Antiretroviral drug class and anaemia risk in the current treatment era among people living with HIV in the USA; a clinical cohort study. BMJ. 2020 March [cited 2023 April 23]; 10(3). Available from: https://bmjopen.bmj.com/content/10/3/e031487.info
- Castleman T, Seumo-Fosso E, Cogill B. Food and Nutrition Implications of Antiretroviral Therapy in Resource Limited Settings. Food and Nutrition Technical Assistance [Internet]. Washington DC: FANTA; 2004 [cited 2023 April 25].20.7.: Available from: https://www.aidsdatahub.org/sites/default/files/resource/food-and-nutrition-implications-antiretroviral-therapy-resource-limited-settings-2004.pdf
- Van Graan AE. Nutritional Management in HIV/AIDS Infection. Cited in Bier D, et al. Nutrition for the primary Care Provider. World Rev Nutr Diet. Karger [Internet]. 2015; [cited: 2023 April 27]; 111: 130-135.
- South African Lancet National Commission. Confronting the right to ethical and accountable quality health care in South Africa: A consensus report. Pretoria: National Department of Health, 2019 [cited 2023 Apr 28]. Available from: https://bhekisisa.org/wp-content/uploads/2019/07/620a9eb9-final-sa-lnc-report.pdf
- Gebru TH, Mekonen HH, Kiros KG. Undernutrition and associated factors among adult HIV/AIDS patients receiving antiretroviral therapy in eastern zone of Tigray, Northern Ethiopia: a cross-sectional study. Arch Public Health [Internet]. 2020 Oct [cited: 2023 Apr 26th];78: 100.Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7559062/
- Khatri S, Amatya A, Shrestha B. Nutritional status and the associated factors among people living with HIV: an evidence from cross-sectional survey in hospital based antiretroviral therapy site in Kathmandu, Nepal. BMC Nutr [Internet]. 2020 Jun [cited: 2023 Apr 27];6: 22. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7294605/
- Misselhorn A, Hendriks SL. A systematic review of sub-national food insecurity research in South Africa: Missed opportunities for policy insights. PLoS One [Internet]. 2017 [cited 2023 April 27th]; 12(8): e0182399. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5567909
References:
- World Health Organisation (WHO), HIV/AIDS: Key Facts, July 2020. Accessed 10 September 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids
- Justiz Vaillant AA, Gulick PG. HIV Disease Current Practice. [Updated 2022 Sep 20]. In: StatPearls [Internet]. Treasure Island (FL): Statpearls Publishing; 2023 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534860.
- Human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS)
- South African Lancet National Commission. Confronting the right to ethical and accountable quality health care in South Africa: A consensus report. Pretoria: National Department of Health, 2019. Available from: https://bhekisisa.org/wp-content/uploads/2019/07/620a9eb9-final-sa-lnc-report.pdf
- AFAO. Australian HIV Statistics. 2023. Accessed 20 April 2023. Available from: https://www.afao.org.au/wp-content/uploads/2022/11/hiv-in-australia-2023.pdf